PUBLIC-POLICY OBJECTIVE FUNCTION: MAXIMIZE MEDIAN HEALTHY LIFE EXPECTANCY AND REAL MEDIAN AFTER-TAX INCOME.
THE LONG-TERM OBJECTIVE: MAXIMIZE PLEASANT CONSCIOUSNESS IN THE UNIVERSE.
THE SHORT-TERM PLAN: SOFTWARE, CAUSAL INFERENCE, ECONOMICS, AND A MEDICALLY CONCERNING NUMBER OF SPREADSHEETS.
HERE ARE THE EXPERIMENTS, SYSTEMS, AND MILDLY UNHINGED PROTOTYPES I'M BUILDING TO TEST THAT IDEA.

WORKING PAPERS
PEER-REVIEWED BY EXACTLY ZERO PEERS. CITED BY FEWER. STILL MATHEMATICALLY CORRECT.

THE 1% TREATY: HARNESSING GREED TO ERADICATE DISEASE
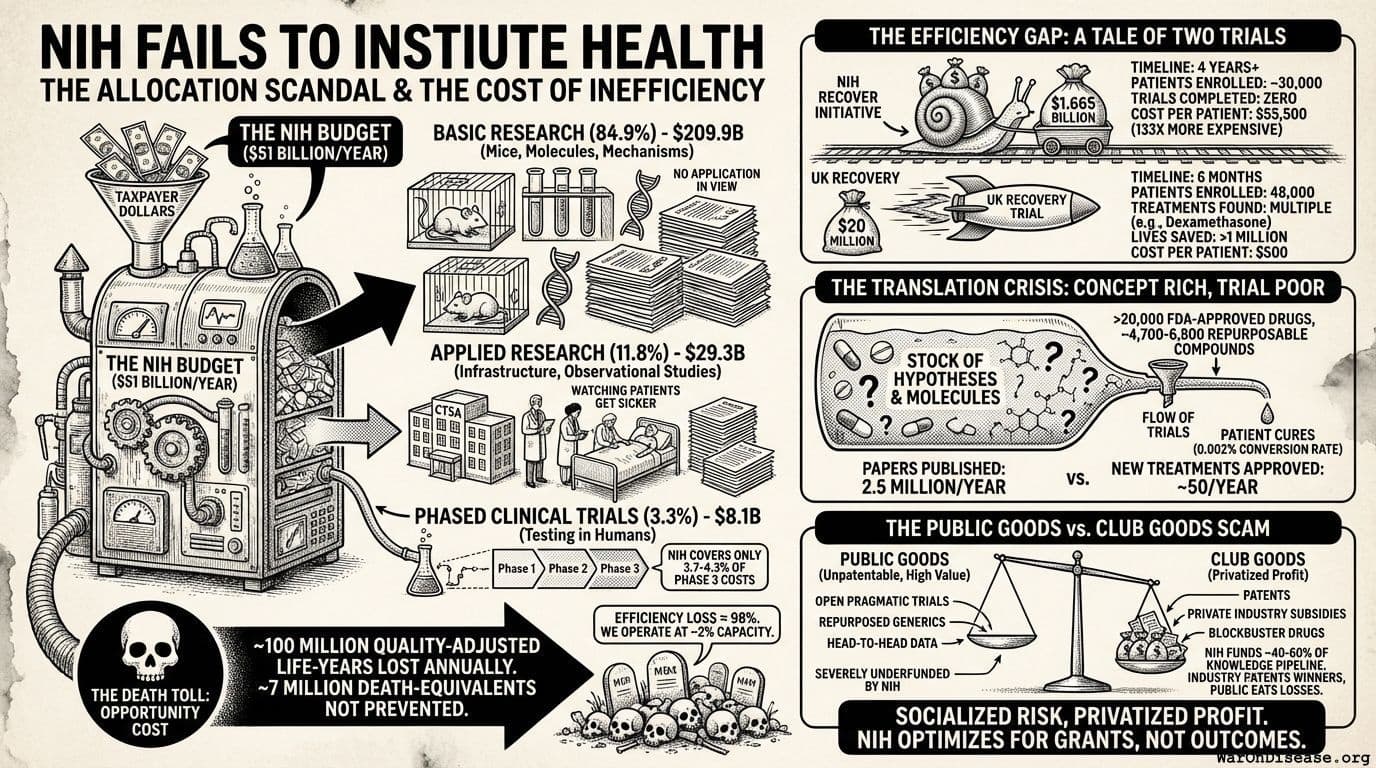
6.65 THOUSAND DISEASES HAVE ZERO FDA-APPROVED TREATMENTS; AT CURRENT TRIAL CAPACITY, EXPLORING THEM TAKES ~443 YEARS. REDIRECTING 1% OF MILITARY SPENDING SCALES CAPACITY 12.3X, CUTTING THE TIMELINE TO ~36 YEARS AND PREVENTING 10.7 BILLION DEATHS. AT $0.00177/DALY, 50.3KX MORE COST-EFFECTIVE THAN THE BEST EXISTING INTERVENTIONS. INCENTIVE ALIGNMENT BONDS MAKE ADOPTION POLITICALLY VIABLE.
ALGORITHMIC PUBLIC ADMINISTRATION: A PROTOCOL FOR REPLACING GOVERNMENT INTERMEDIARIES WITH DETERMINISTIC FUNCTIONS
A PROTOCOL COMBINING FIVE PRIMITIVES (TRANSPARENT LEDGER, PREFERENCE AGGREGATION, EVIDENCE ENGINE, IDENTITY VERIFICATION, AUTOMATED MONETARY POLICY) TO REPLACE MECHANICAL GOVERNMENT AGENCY FUNCTIONS, ELIMINATING ADMINISTRATIVE INTERMEDIATION COSTS WHILE PRESERVING DEMOCRATIC CONTROL.

THE PRICE OF POLITICAL CHANGE: A COST-BENEFIT FRAMEWORK FOR POLICY INCENTIVIZATION
WHAT'S THE MAXIMUM COST TO ACHIEVE ANY POLICY CHANGE THROUGH LEGAL DEMOCRATIC CHANNELS? $25B FOR THE US, $200B GLOBALLY. FOR HIGH-VALUE REFORMS LIKE MILITARY-TO-HEALTH REALLOCATION, THIS YIELDS ROI EXCEEDING 400,000:1.

UBIQUITOUS PRAGMATIC TRIAL IMPACT ANALYSIS: HOW TO PREVENT A YEAR OF DEATH AND SUFFERING FOR 84 CENTS
ONLY 15 DISEASES/YEAR GET THEIR FIRST TREATMENT EACH YEAR. WITH 6.65 THOUSAND DISEASES LACKING EFFECTIVE TREATMENTS, THE BACKLOG WOULD TAKE 443 YEARS TO CLEAR. INTEGRATING PRAGMATIC TRIALS INTO STANDARD HEALTHCARE INCREASES TRIAL CAPACITY 12.3X, CUTTING THAT TIMELINE FROM 443 YEARS TO 36 YEARS. THE AVERAGE UNTREATED DISEASE GETS A TREATMENT 212 YEARS EARLIER, SAVING 10.7 BILLION DEATHS AT $0.842 PER YEAR OF HEALTHY LIFE SAVED.

THE CONTINUOUS EVIDENCE GENERATION PROTOCOL: TWO-STAGE VALIDATION (RWE → PRAGMATIC TRIALS)
WE PRESENT THE PREDICTOR IMPACT SCORE (PIS), A NOVEL COMPOSITE METRIC OPERATIONALIZING BRADFORD HILL CAUSALITY CRITERIA FOR AUTOMATED SIGNAL DETECTION FROM AGGREGATED N-OF-1 OBSERVATIONAL STUDIES. COMBINED WITH PRAGMATIC TRIAL CONFIRMATION (BASED ON EVIDENCE FROM 108+ EMBEDDED TRIALS), THIS TWO-STAGE FRAMEWORK WOULD GENERATE VALIDATED OUTCOME LABELS AT 44.1X LOWER COST THAN TRADITIONAL PHASE III TRIALS. THIS ENABLES CONTINUOUS, POPULATION-SCALE PHARMACOVIGILANCE AND PRECISION DOSING RECOMMENDATIONS.


EARTH OPTIMIZATION PRIZE PROTOCOL: TECHNICAL SPECIFICATION
TECHNICAL SPECIFICATION FOR INTEROPERABLE OUTCOME PRIZE POOLS STRUCTURED AS A DOMINANT ASSURANCE CONTRACT. COVERS CROSS-POOL PROOF-OF-PERSONHOOD, A PERMISSIONLESS POOL REGISTRY, VOTE AND PRIZE TOKEN MECHANICS, DIRECT CROSS-POOL CLAIMS, TAMPER-EVIDENT SCOREBOARD AGGREGATION, AND A TERMINAL METRIC ORACLE INCLUDING DECENTRALIZED SURVEYS.


CHOOSE YOUR OWN EARTH: A WORLD WITHOUT THE POLITICAL DYSFUNCTION TAX, OR TERMINAL PARASITIC LOAD IN 15 YEARS
YOUR DESTRUCTIVE ECONOMY (MILITARY SPENDING PLUS CYBERCRIME) IS ALREADY 11.5% OF GDP AND GROWING FASTER THAN YOUR PRODUCTIVE ECONOMY. AT CURRENT RATES, IT REACHES THE SOVIET COLLAPSE THRESHOLD IN 8 YEARS AND EXCEEDS PRODUCTIVE OUTPUT IN 15. THIS PAPER MODELS TWO GDP TRAJECTORIES: THE OPTIMIZED PATH UNDER MILITARY-TO-MEDICAL REALLOCATION, AND THE DEFAULT PATH TO CIVILIZATIONAL COLLAPSE.

INCENTIVE ALIGNMENT BONDS: MAKING PUBLIC GOODS FINANCIALLY AND POLITICALLY PROFITABLE
GOVERNMENT SPENDING IS OPTIMIZED FOR LOBBYING INTENSITY, NOT NET SOCIETAL VALUE. PROGRAMS WITH 100:1 BENEFIT-COST RATIOS GET BILLIONS WHILE PROGRAMS WITH NEGATIVE RETURNS GET HUNDREDS OF BILLIONS. INCENTIVE ALIGNMENT BONDS FLIP THIS BY CREATING A CAPITAL POOL THAT REWARDS POLITICIANS (VIA CAMPAIGN SUPPORT AND POST-OFFICE OPPORTUNITIES) FOR FUNDING HIGH-NSV PROGRAMS OVER LOW-NSV ALTERNATIVES. THE RESULT: PUBLIC GOOD BECOMES PRIVATE PROFIT FOR BOTH INVESTORS AND ELECTED OFFICIALS.

THE INVISIBLE GRAVEYARD: QUANTIFYING THE MORTALITY COST OF FDA EFFICACY LAG
AFTER PROVING A DRUG IS SAFE, THE FDA REQUIRES 8.2 YEARS TO PROVE IT WORKS BEFORE PATIENTS CAN ACCESS IT. WE ESTIMATE THIS DELAY COST 102 MILLION DEATHS AMONG PEOPLE WAITING FOR APPROVED DRUGS (1962-2024). THE HUMAN COST IN DEATH AND DISABILITY OF BLOCKING GOOD DRUGS IS 3.07K HIGHER THAN THE COST OF APPROVING BAD ONES.



THE OPTIMAL BUDGET GENERATOR: A CAUSAL INFERENCE PROTOCOL FOR MAXIMIZING MEDIAN HEALTH AND WEALTH THROUGH PUBLIC GOODS FUNDING
THE OPTIMAL BUDGET GENERATOR (OBG) USES CAUSAL INFERENCE, DIMINISHING RETURNS MODELING, AND COST-EFFECTIVENESS EVIDENCE TO DETERMINE OPTIMAL PUBLIC GOODS FUNDING LEVELS THAT MAXIMIZE TWO WELFARE METRICS: REAL AFTER-TAX MEDIAN INCOME GROWTH AND MEDIAN HEALTHY LIFE YEARS. FOR EACH SPENDING CATEGORY, OBG ESTIMATES AN OPTIMAL SPENDING LEVEL (OSL) AND PRODUCES A GAP ANALYSIS SHOWING WHERE CURRENT GOVERNMENT BUDGETS ARE OVER- OR UNDERFUNDED RELATIVE TO EVIDENCE-BASED BENCHMARKS. THE BUDGET IMPACT SCORE (BIS) MEASURES CONFIDENCE IN EACH RECOMMENDATION BASED ON THE QUALITY OF CAUSAL EVIDENCE.

THE OPTIMAL POLICY GENERATOR: A CAUSAL INFERENCE PROTOCOL FOR MAXIMIZING MEDIAN HEALTH AND WEALTH THROUGH PUBLIC POLICY
THE OPTIMAL POLICY GENERATOR (OPG) PRODUCES SYSTEMATIC PUBLIC POLICY RECOMMENDATIONS FOR JURISDICTIONS AT ANY LEVEL (COUNTRY, STATE, CITY), GENERATING PRIORITIZED ENACT/REPLACE/REPEAL/MAINTAIN RECOMMENDATIONS TO MAXIMIZE REAL AFTER-TAX MEDIAN INCOME GROWTH AND MEDIAN HEALTHY LIFE YEARS, BASED ON QUASI-EXPERIMENTAL EVIDENCE FROM CENTURIES OF POLICY VARIATION DATA.

OPTIMOCRACY: CAUSAL INFERENCE ON CROSS-JURISDICTIONAL POLICY DATA TO MAXIMIZE MEDIAN HEALTH AND WEALTH
THOUSANDS OF JURISDICTIONS HAVE MADE DIFFERENT POLICY AND BUDGET CHOICES OVER DECADES, CREATING A NATURAL EXPERIMENT. OPTIMOCRACY APPLIES CAUSAL INFERENCE TO THIS CROSS-JURISDICTIONAL TIME-SERIES DATA TO IDENTIFY WHICH POLICIES PREDICT ABOVE-AVERAGE MEDIAN INCOME AND HEALTHY LIFE YEARS. IT THEN PUBLISHES EVIDENCE-BASED RECOMMENDATIONS FOR EVERY MAJOR VOTE, TRACKS POLITICIAN ALIGNMENT, AND FUNDS ALIGNED CANDIDATES VIA SUPERPAC, MAKING SUBOPTIMAL POLICY POLITICALLY EXPENSIVE WHILE PRESERVING DEMOCRATIC STRUCTURES.





WISHOCRACY: SOLVING THE DEMOCRATIC PRINCIPAL-AGENT PROBLEM THROUGH PAIRWISE PREFERENCE AGGREGATION
REPRESENTATIVE DEMOCRACY SUFFERS FROM AN INESCAPABLE PRINCIPAL-AGENT PROBLEM WHERE ELECTED OFFICIALS' INCENTIVES DIVERGE FROM CITIZEN WELFARE. WISHOCRACY INTRODUCES RAPPA (RANDOMIZED AGGREGATED PAIRWISE PREFERENCE ALLOCATION), WHICH AGGREGATES CITIZEN PREFERENCES THROUGH COGNITIVELY TRACTABLE PAIRWISE COMPARISONS AND CREATES ACCOUNTABILITY VIA CITIZEN ALIGNMENT SCORES THAT CHANNEL ELECTORAL RESOURCES TOWARD POLITICIANS WHO ACTUALLY REPRESENT WHAT CITIZENS WANT.
SO DO YOU LIKE STUFF?
I BUILT PLATFORMS TO ANALYZE HEALTH DATA AT SCALE. CHRONIC ILLNESS REMAINS UNIMPRESSED.
OBSERVATIONAL STUDIES
AGGREGATED & ANALYZED TO DETERMINE EFFECTS OF FOODS, DRUGS, AND SUPPLEMENTS
META-ANALYSES
COVERAGE FOR CONDITION/TREATMENT PAIRS USING OPEN-SOURCE PLATFORMS
ACTIVE PROJECTS
OPEN-SOURCE PLATFORMS FOR HEALTH DATA ANALYSIS AND POLICY RESEARCH
WHAT I'M BUILDING
WHAT IF CLINICAL TRIALS COST $500 INSTEAD OF $41,000 PER PARTICIPANT?
82× CHEAPER. 8× FASTER. 416M LIVES SAVED. HERE'S WHAT I'M BUILDING TO MAKE IT HAPPEN.

Optimitron
An open-source platform that uses causal inference to figure out which policies actually save lives instead of just sounding good at press conferences. Analyzed 11 natural experiments and 14 policy areas across 50+ years. Found that Singapore gets better health outcomes at 4.1% GDP while the US spends 17.3% and somehow does worse. Portugal decriminalized drugs and deaths dropped 94%. Norway rehabilitates prisoners and recidivism dropped to 20% vs America's 76%. All of this data is freely available. Policymakers remain committed to vibes-based governance.
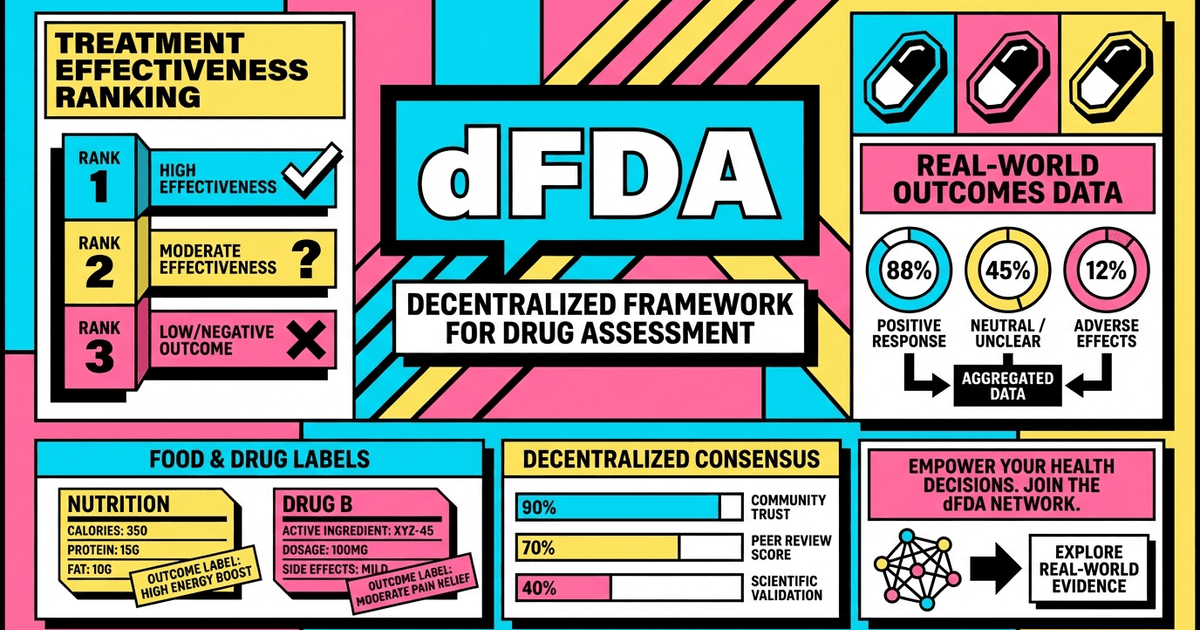
Decentralized FDA
A system optimized for saving lives rather than avoiding lawsuits. 50,000+ observational studies analyzed. Meta-analyses for 90%+ of condition-treatment pairs. Treatment rankings for 100+ conditions. The current FDA approval process takes 10+ years and costs $2.6B per drug. During that time, between 11,000 and 115,000 people die who could have been saved if the drug had been approved immediately. There are roughly 1.16 quadrillion possible drug combinations we haven't tested. At the current pace, we'll finish testing them all in approximately never. The dFDA could accelerate clinical discovery by 80X. Which, if my math is correct, means we could map the entire space of possible treatments in about 45 minutes.
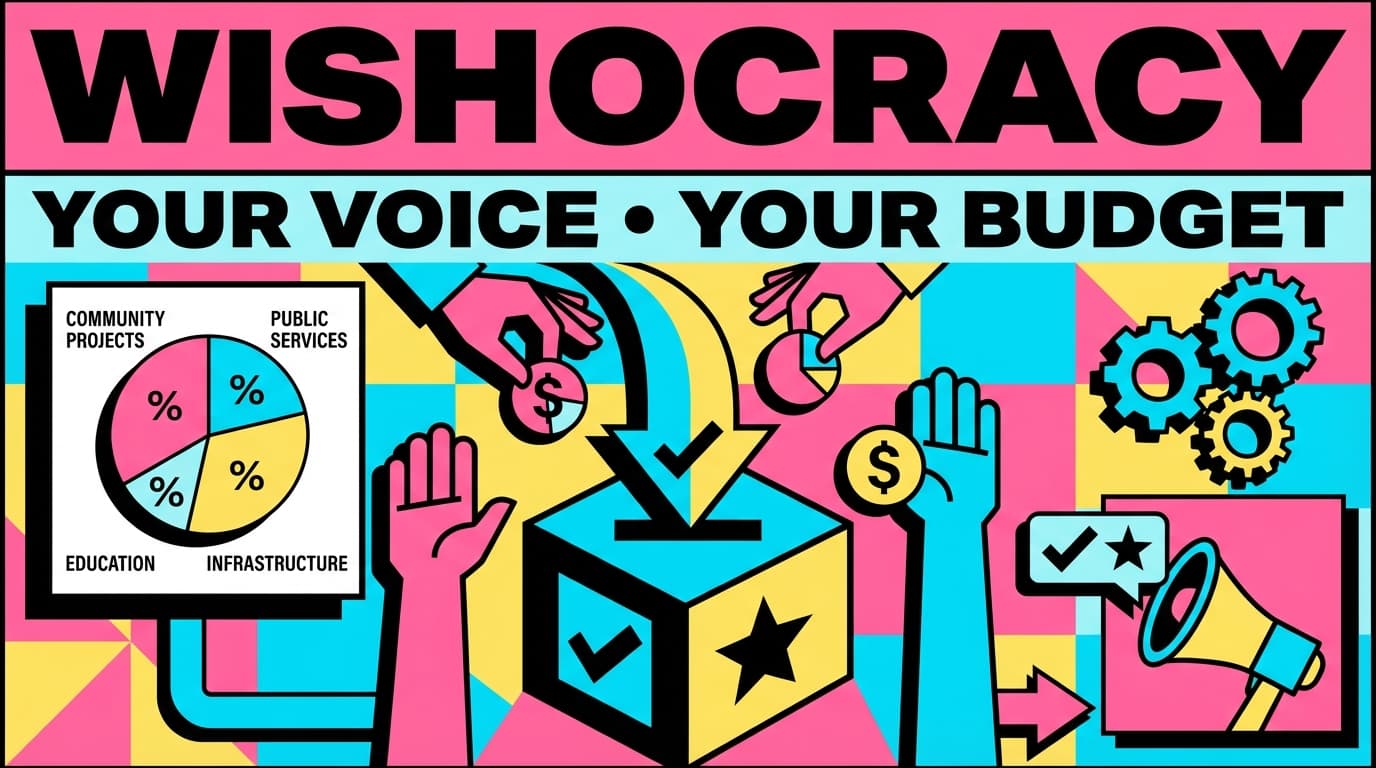
Wishocracy
A governance mechanism called RAPPA that decomposes impossible budget decisions into simple pairwise slider comparisons. You spend 5-10 minutes doing ~20 comparisons. The eigenvector math does the rest. The US spends $886B on military vs $47B on NIH despite medical research having a 45:1 benefit-cost ratio vs military's 0.7:1. When Porto Alegre let citizens set priorities, water access went from 75% to 98% and schools quadrupled. Taiwan used pairwise comparison tools to resolve a 4-year regulatory deadlock. The math works. The political will remains theoretical.

How to End War and Disease
I helped an alien named WISHONIA write an instruction manual for humanity about how to stop spending 40x more on building Skynet than on curing the diseases that are dissolving you. The alien has been watching your planet since 1945 and is very concerned. Available in paperback, Kindle, free online, and as an audiobook podcast.
Global Survey on the 1% Treaty
Redirect 1% of global military spending to health research. Save 416 million lives. 700× more effective than current spending. I sent this proposal to everyone with the power to implement it. They have enthusiastically ignored me. When your last name is Sinn, you take validation wherever you can find it.
Think by Numbers
Data-driven policy analysis. Articles like 'The War on Drugs Increases Drug Deaths' and 'We Spend More on Corporate Welfare Than Social Welfare.' 2 million people read these. The policy remains exactly the same. But I made some really compelling charts and I stand by them.
CureDAO
A DAO focused on clinical research. That's a lot of technical jargon, so let me translate: imagine if Wikipedia and a clinical trial had a baby that was raised by blockchain. The result is a platform where anyone can contribute to medical research without needing permission from a committee of very tired people in lab coats.

RECENT RESEARCH
192+ PUBLICATIONS ON CLINICAL RESEARCH, POLICY ANALYSIS, AND THE OPTIMAL ALLOCATION OF SOCIETAL RESOURCES.


CONTRIBUTE DATA. DISTURB THE OBJECTIVE FUNCTION.
TWO SMALL WAYS TO HELP DECIDE WHAT HUMANITY SHOULD OPTIMIZE BEFORE THE CURRENT ALGORITHM SPENDS EVERYTHING ON YACHTS AND MISSILES.